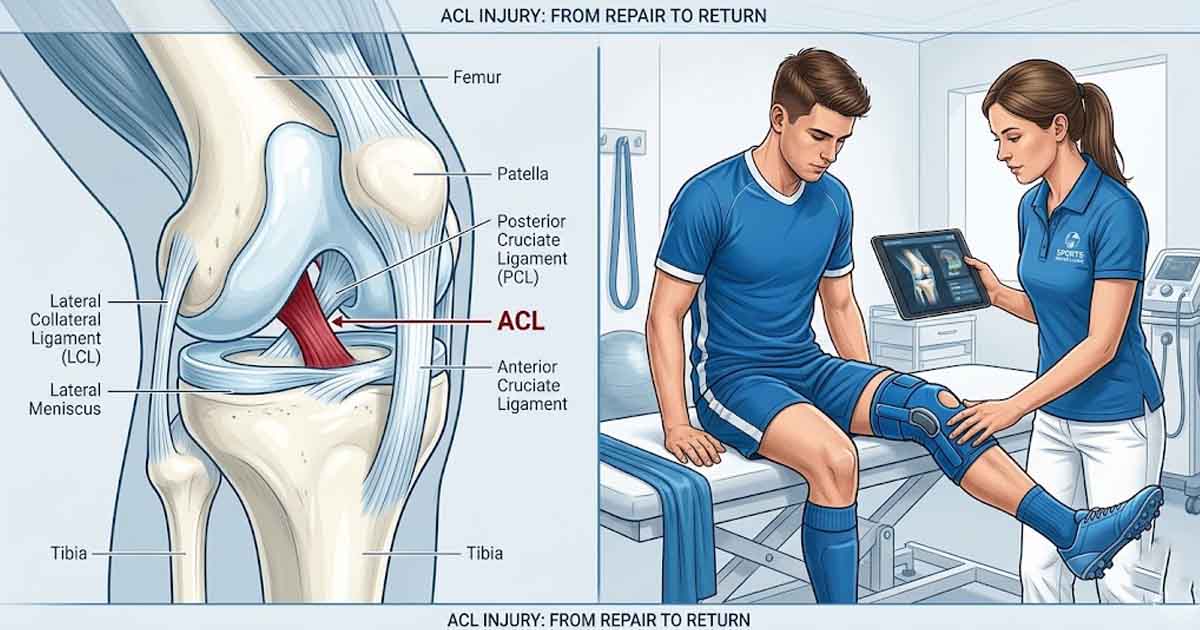
The anterior cruciate ligament — known universally in sport simply as the ACL — is a roughly 35mm band of dense connective tissue in the center of the knee joint. Its function is to control the forward movement of the tibia relative to the femur and to prevent excessive rotation of the knee joint. It is not a large structure by anatomical standards. Yet its failure — the terrifying pop that echoes around a stadium when it ruptures — has shaped the careers of countless professional athletes and generated an entire subspecialty within sports medicine devoted to its repair.
ACL injuries in football — both association football and American football — are among the most common and most consequential injuries in professional sport. Understanding the biology of the injury, the options for surgical repair, the structure of rehabilitation, and the realistic timeline for return to play is essential for athletes, coaches, parents, and anyone who follows the careers of professional players through their injury absences.
How ACL Injuries Happen
The majority of ACL injuries in football occur without contact — approximately 70% of ACL tears happen when the player is decelerating, changing direction, or landing from a jump. The mechanism is typically a planting of the foot combined with a sudden change of direction, causing the knee to buckle inward in what sports medicine professionals call a valgus collapse.
Contact ACL injuries — such as those caused by a tackle hitting the side of the knee — also occur, particularly in American football where high-speed impacts to the lower extremity are common. Female athletes are statistically at significantly higher risk of ACL injury than males in equivalent sports, a disparity attributed to biomechanical, hormonal, and neuromuscular factors.
Surgical Options: Graft Types and Their Trade-offs
Once an ACL is torn, it does not heal spontaneously in most cases. Surgical reconstruction is the standard treatment for professional athletes who wish to return to competitive sport. The surgery involves replacing the torn ligament with a graft — a section of tendon harvested from either the patient's own body or from a donor. The three most commonly used graft types in elite sport are the patellar tendon graft, the hamstring tendon graft, and the quadriceps tendon graft.
Each graft type carries its own profile of advantages and disadvantages. The patellar tendon graft — bone-to-bone fixation — has traditionally been favored for high-demand athletes because of its strength and reliable integration into the knee joint, but it carries a higher risk of anterior knee pain. The hamstring graft offers a less painful donor site but may have slightly lower initial strength. The quadriceps graft is increasingly favored in recent sports medicine literature for its strength-to-morbidity ratio, though surgical technique expertise requirements are higher.
The Rehabilitation Timeline
ACL rehabilitation following surgical reconstruction is a phased process that typically runs nine to twelve months for elite athletes before competitive return, though some cases — particularly complex multi-ligament injuries or revisions — can require eighteen months or longer. The phases of rehabilitation are structured around tissue healing biology: the graft initially integrates into the knee through a process called ligamentization, during which it is at its most vulnerable.
Phase one, covering roughly the first six weeks post-surgery, focuses on controlling swelling, restoring range of motion, and beginning quadriceps activation. Phase two, from weeks six to twelve, progressively loads the graft through resistance training. Phase three, from months three to six, introduces sport-specific movement patterns. Phase four, from months six to nine, incorporates full speed running and sports-specific drills. Return to competitive play is typically sanctioned when objective criteria — including strength symmetry between the injured and uninjured leg — are met, regardless of the calendar timeline.
Return-to-Play Criteria and Re-injury Risk
The re-injury rate following ACL reconstruction is a sobering aspect of the evidence base. Studies suggest that between 20 and 25 percent of athletes who return to competitive sport following ACL surgery sustain another ACL injury — either to the reconstructed knee or, more commonly, to the contralateral knee — within five years of return. This elevated re-injury risk reflects residual neuromuscular deficits, psychological factors, and the simple reality that the reconstructed ligament never fully replicates the mechanical properties of the original structure.
Return-to-play criteria have therefore become increasingly sophisticated, moving beyond simple time-from-surgery calendars to incorporate battery of functional tests measuring limb symmetry, reaction time, and sport-specific movement quality. Clubs and sports medicine teams that implement rigorous return-to-play screening report lower re-injury rates, though eliminating re-injury risk entirely remains beyond the current state of the science.


Add a Comment